The term
spirometry is defined as the use of a spirometer to obtain
measurements of breathing capacity, however the term is used
more generically to mean Lung or Pulmonary Function Testing
(PFT) to acquire information about the lung volumes, flow rates
and the physiological function.
The reason
for assessing someone's Pulmonary Function will determine
exactly what sort of PFT will be required. Sometimes just the
most basic test, a Peak Flow, will suffice and provide enough
information of a patient's condition for the clinician. Mostly a
whole bselection of investigations will be required to provide
more information to enable an accurate diagnosis or prognosis.
Questionnaires can also provide useful information by asking
about any symptoms, frequency of episodes and if or when
Bronchodilators were last used (The use of Bronchodilators, such
as Salbutamol, can often affect PFT results).
When
performing spirometry the clinician must try and ensure that
maximal effort is obtained at each attempt as sub-par effort
will limit the clinical value of the tests. Whatever
procedures are indicated they are always compared to a set of
Normal Values. These values take into consideration common
factors such as gender, age, height and race, on occasion
other parameters are used such as Body Surface Area (BSA).
There are three main sets of Normal Values:
1.
European
Respiratory Society (ERS) 1993 regression values, are
recommended by American Thoracic Society/European Respiratory
Society (ATS/ERS) Task Force as the 'Standardisation of Lung
Function testing for Europeans'. These tables are the most
widely used in Europe and elsewhere and were published in 1993.
2.
National Health and Nutrition Examination
Survey (NHANES) in it's current form of NHANES III, is
recommended for ethnically appropriate individuals by ATS/ERS
and is used in the Americas and elsewhere. These tables were
published in 1999.
3.
Global Lungs Quanjer (GLI-2012)
regressions are based on the NHANES III but use an added method
(Lambda-mu-sigma (LMS)) to process thenormal values. These
values were published in 2008, accepted by ERS in 2010 but are
not widely used.
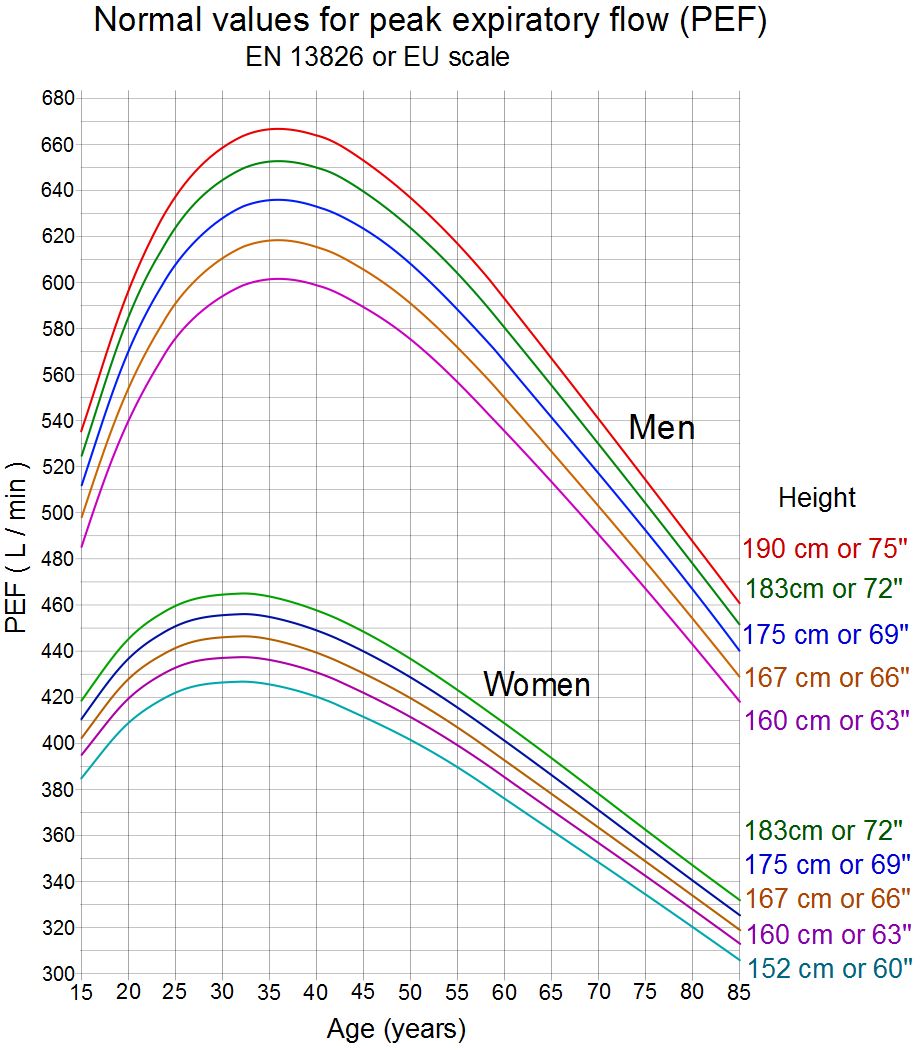
Peak Flow
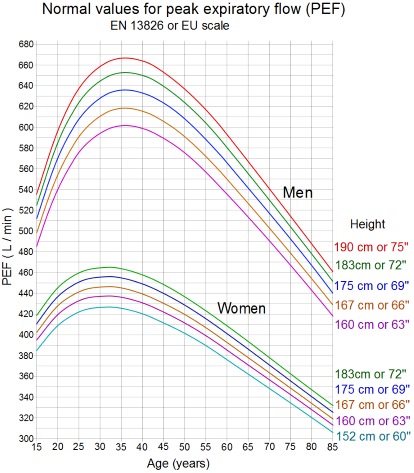 The most
commonest PFT testing that can be done is the Peak Flow. A Peak
Flow Meter is a small, portable handheld device that is quite
inexpensive. It's purpose is to record a person's Peak
Expiratory Flow Rate (PEF or PEFR) or the fastest that a person
can breathe out. This measurement is recorded in litres per
minute.
The most
commonest PFT testing that can be done is the Peak Flow. A Peak
Flow Meter is a small, portable handheld device that is quite
inexpensive. It's purpose is to record a person's Peak
Expiratory Flow Rate (PEF or PEFR) or the fastest that a person
can breathe out. This measurement is recorded in litres per
minute.
Procedure:
The person is instructed to inhale fully, place the tube in the
mouth and exhale as hard as they can, so 'take a deep breath and
blow out as hard as you can' should elicit maximum results. This
procedure can repeated a number of times (best of three) until a
consistent result is obtained. Many repeated attempts must be
avoided due to fatigue with a resultant drop in the score.
This item is
an ideal way to monitor some respiratory disorders quickly and
easily in a doctors Practice or even at home, over a period of
time keeping a log of the results to see if any trend is
apparent, such as low scores at dawn/dusk possibly relating to
pollen counts.
Spirometry
Spirometry is
probably the most commonest clinical form of PFT. The type of
machine varies and can be either a 'Bellows' type or a Strain
gauge variant, although they look different they perform the
same test. Spirometry records expelled volume over time and from
this certain measurements may be taken.
Procedure:
The person is instructed to take a deep breath and then to blow
out as hard as they can and to continue to empty their lungs
until told to stop (usually 6 seconds). In some cases a longer
period is required for subjects to empty their lungs completely
and care must be taken when this is required, especially the
elderly and children.
A slight
amendment to the procedure is required if the Vital Capacity is
to be recorded as apposed to the Forced Vital Capacity, in this
case the subject is instructed to take a deep breath and then in
their own time, without forcing the air, the empty their lungs
completely and then stop. With this technique people can usually
empty their lungs for up to 12 seconds.
Peak
Expiratory Flow (PEF) can be recorded as the calculated fastest
velocity of exhaled breath.
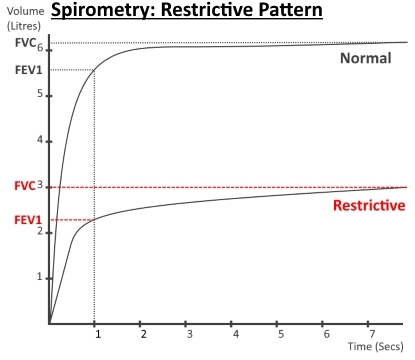
Forced
Expiratory Volume in 1 second (FEV1) is calculated as
the volume that was expired at 1 second once breathing out was
commenced. Further FEV measurements can be recorded but these
are not done routinely such as FEV0.5, FEV3
and FEV6 (½, 3 and 6 seconds
respectively).
Forced Vital
Capacity (FVC) and Vital Capacity (VC), this records total
volume of air expelled with slightly different techniques. If
there is a difference between VC and FVC it usually indicates a
collapse of the small airways.
FEV1/FVC
Ratio (Tiffenau-Pinelli Index) is a calculation comparing the
FEV1 to the FVC and expressed as a percentage.
Forced
Expiratory Flow at 25%-75% (FEF25-75) also called the
Maximum Mid-Expiratory Flow calculates the ratio of expired flow
between 25% volume and 75% volume. This measurement was used to
aid detection of obstruction in the small airways but has since
been shown to correlate with the conventional measurements of
FEV1, FVC, PEF and Tiffenau-Pinelli Index (http://dx.doi.org/10.1183/09031936.00128113)
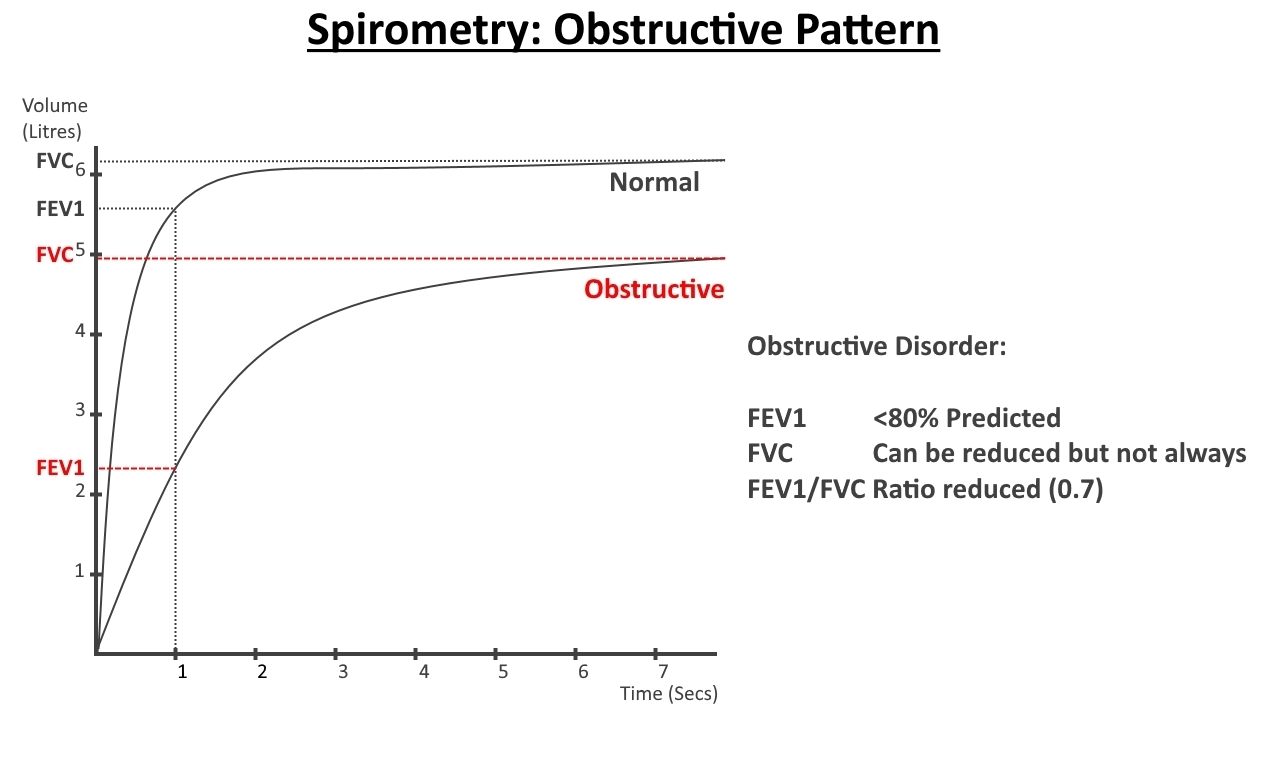
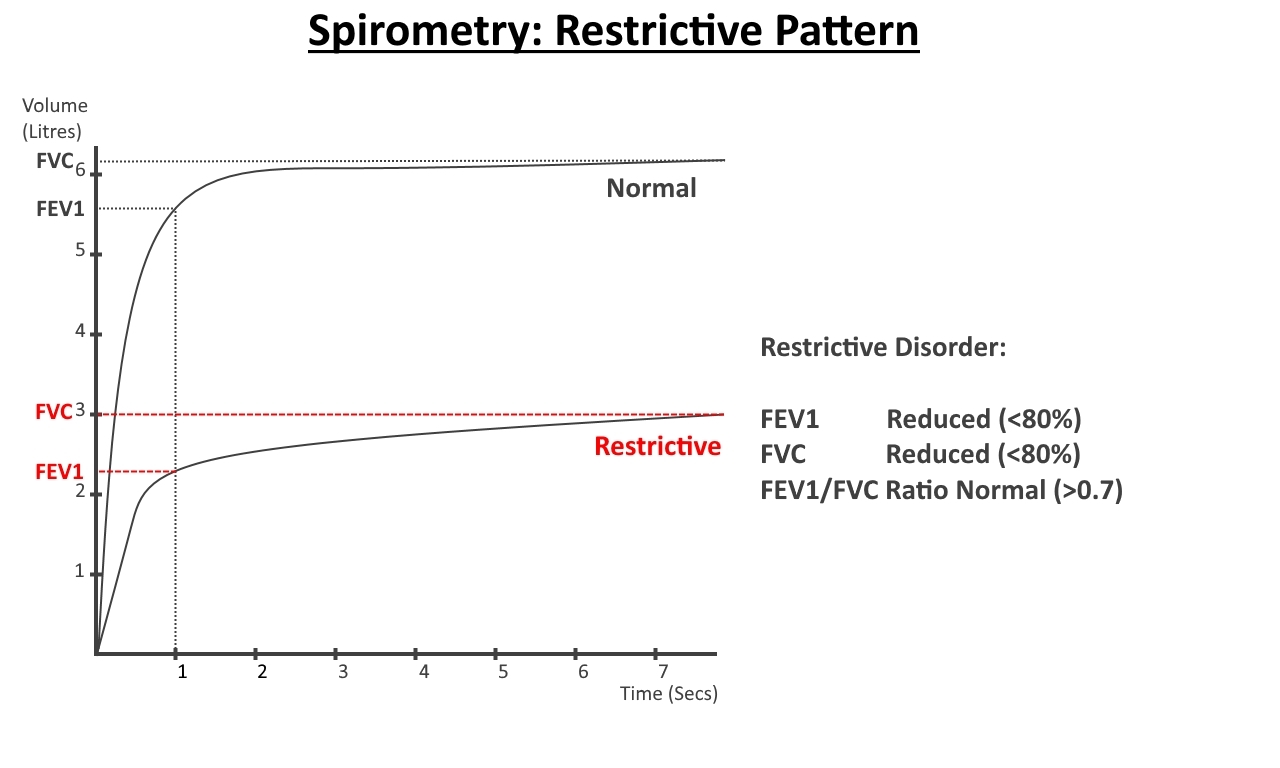
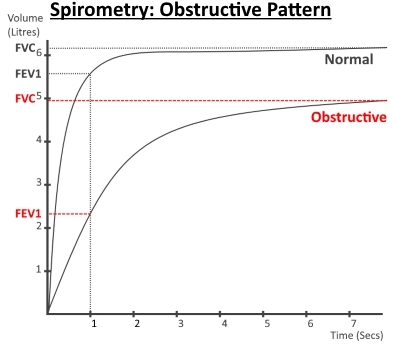
The results
of this should be able to differentiate between normal,
obstructive or restrictive spirometry.
|
Normal |
Obstructive |
Restrictive |
|
|
|
|
| FEV1 |
Normal |
Reduced |
Reduced |
| FVC/VC |
Normal |
Normal or Reduced
|
Reduced |
| Tiffenau-Pinelli
Index (FEV1/FVC) |
Normal |
Reduced |
Normal |
| Peak
Expiratory Flow |
Normal |
Reduced |
Normal or Reduced
|
|
|
|
|
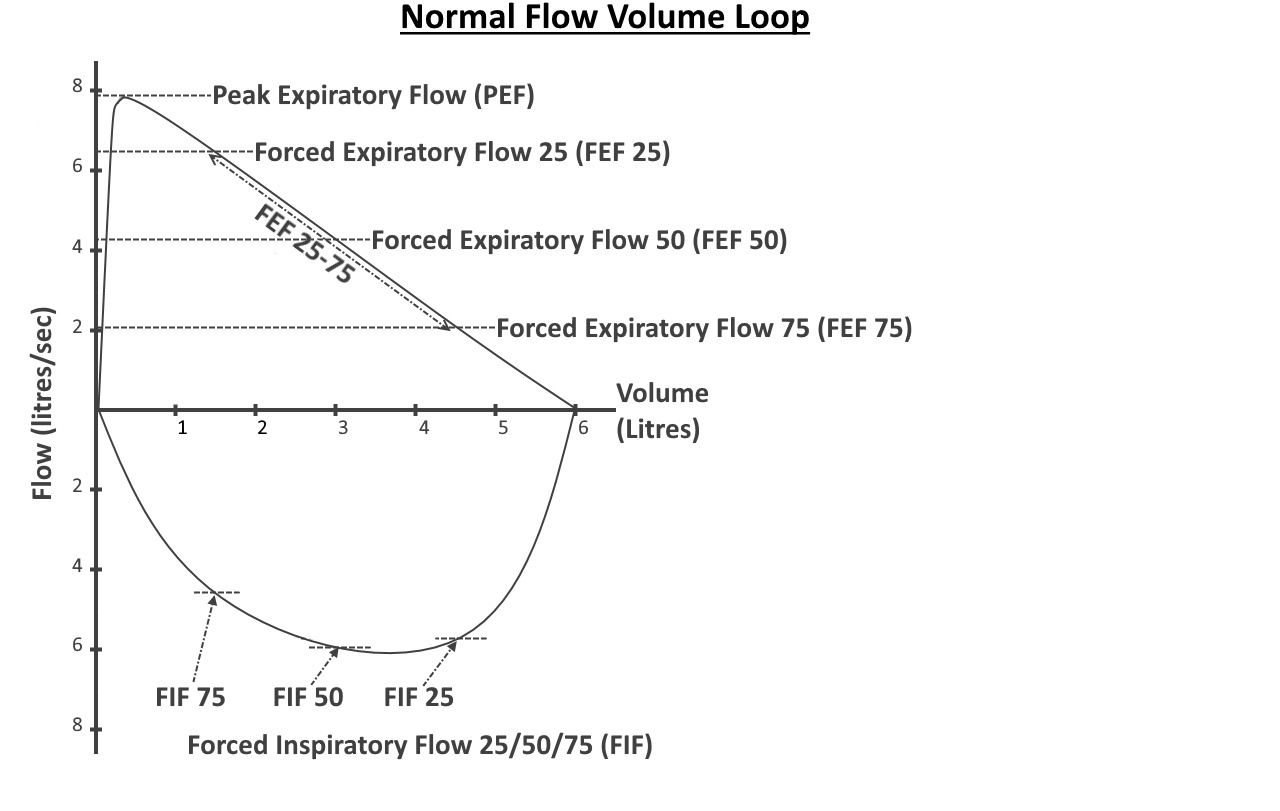
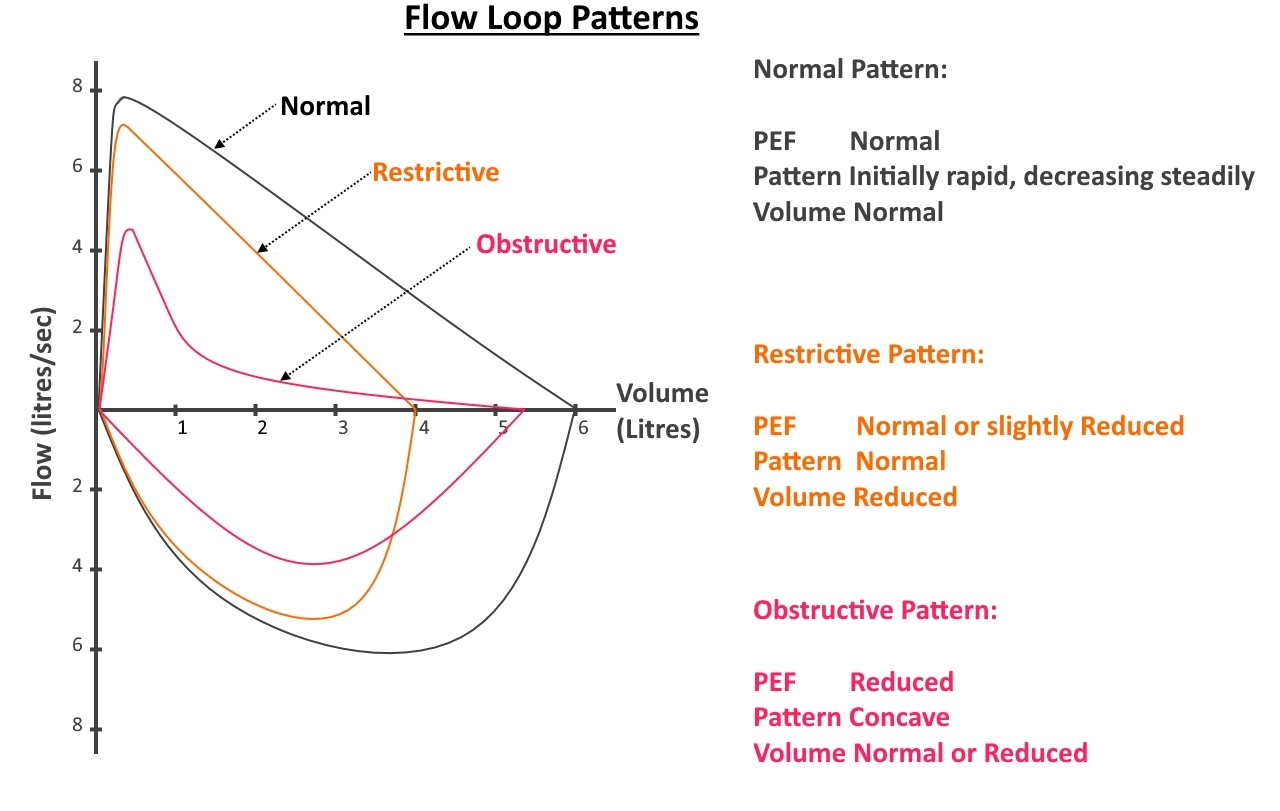
Flow Volume
Loop (Shortened to Floop or Flow Loop)
As previously
explained regular spirometry plots volume of air exhaled (at
maximum effort) against time, a flow loop plots the rate of
expiration (usually as litres per second) against volume
(litres) and then also records the same parameters on
inhalation. This data is represented graphically and forms a
'loop' (see diagram). There are multiple measurements that can
be recorded from this technique and these are listed below.
Procedure:
The initial procedure is the same as for regular spirometry
however when the air is fully expelled from the lungs (the flow
rate reduces to zero) the subject is then instructed to fully
inspire (breath in) maximally at maximum effort. The test is
complete once the inspiration is finished, noted again by the
flow rate reducing to zero.
To the
trained eye the shape of the flow loop can tell immediately if
the test has been performed correctly and can illustrate various
pathologies. The peak expiration is recorded in less than half a
second and then the flow rate reduces until it reaches zero,
this is the point where the subject has fully expelled all the
inspired air. The subject then forcefully breathes in and the
second half of the flow loop is recorded until the flow rate
reduces to zero and then the test is completed. A few more
attempts are then made to ensure consistency in the test
results.
Peak
Expiratory Flow Rate (PEFR) is the maximum rate at which the air
is expelled, this is thought to indicative of the air expelled
from the large airways (trachea & main bronchi).
Forced
Expiratory Flow at 25% (FEF25) expresses the flow
rate at 25% of the total expired volume. Assuming maximal effort
is given this measurement can give some information on the
medium to large sized bronchi.
Forced
Expiratory Flow at 50% (FEF50) is the flow rate when
half the total capacity is expired and should be less than FEF25.
This can indicate the condition of the small to medium airways.
Forced
Expiratory Flow at 75% (FEF75) is the flow rate when
75% of the maximum capacity is reached, this should be less than
FEF25 and FEF50. This measurement can
provide information on the small airways. Most chronic pulmonary
airway diseases show up in the small airways initially so the
latter part of expiration is affected.
Forced
Expiratory Flow 25-75% (FEF25-75) is the mean flow
between these two points and can be quite important as this
measurement will also decline in many respiratory diseases.
Forced
Inspiratory Flow at 25%, 50% and 75% (FIF25, FIF50
& FIF75) are the flow rates of inspiration at a
certain percentage of the total inspired volume. These
measurements are less important in assessing small airway
diseases and can provide some information on upper airway
obstructions (pharynx, larynx, mouth and vocal chords).
Peak
Inspiratory Flow Rate (PIFR) is the fastest flow rate on
inspiration.
Forced
Expiratory Time (FET) is the time taken to exhale a full breath.
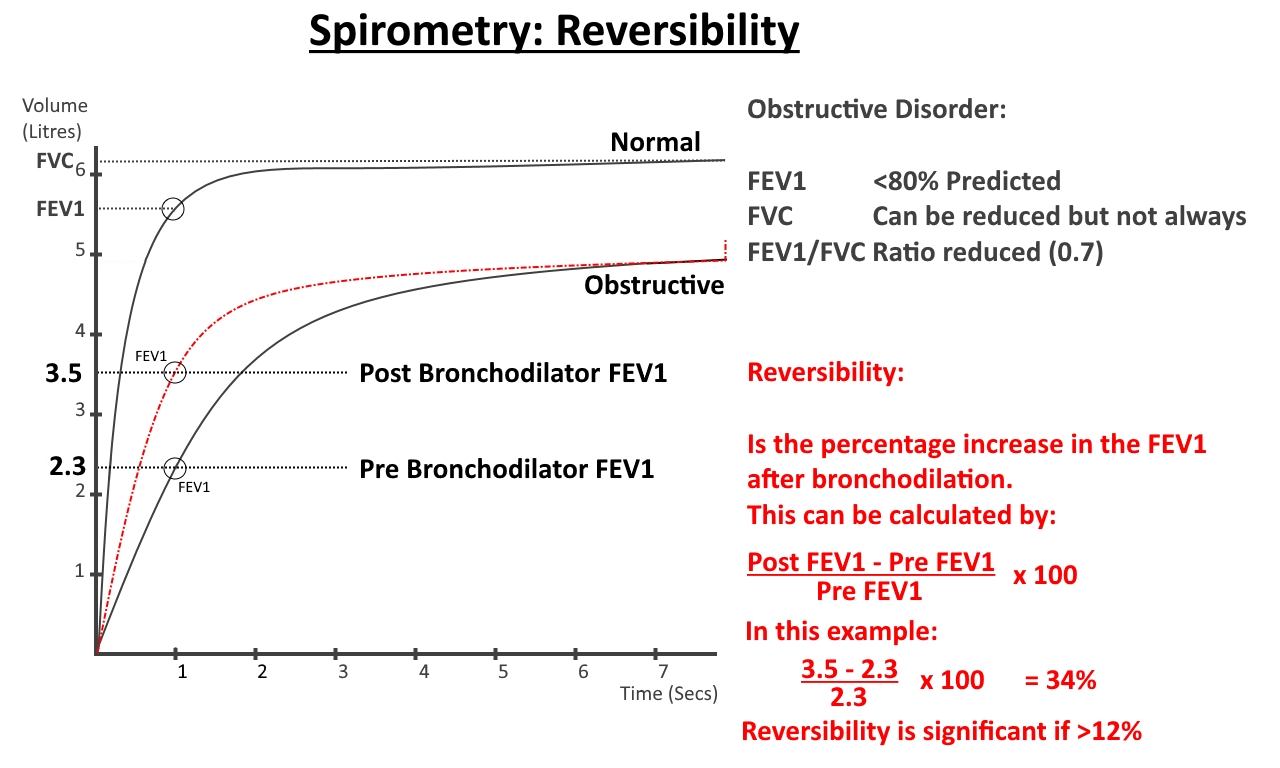
Spirometry
and Reversibility Testing
Obstructive
airways diseases have many causes and performing reversibility
testing with spirometry may provide support for a diagnosis of
reversible asthma. Normal spirometry is performed and if there
is a reduction in the FEV1 or the Tiffenau-Pinelli
Index (FEV1/FVC ratio) then a short acting
bronchodilator is administered and spirometry is repeated again.
Any changes to the results are noted.
If there is
an increase of >12% (at least 200ml) in the FEV1
after the bronchodilation then this indicates a reversible
airflow obstruction and supports the diagnosis of asthma. It
also gives an predictive indication of a good response to an
inhaled corticosteroid.
The absence
of a reversible airways obstruction does not exclude the
diagnosis of asthma and further different testing can be done.
Challenge
Spirometry
In some
subjectively symptomatic patients there is no obvious
abnormality seen in spirometry regularly and this may result in
a normal result at the time of testing. Some form of challenge
or provocation may be required to elicit a change and confirm
the presence of asthma. This can either be done;
a. Directly (using agents that directly
constrict smooth airway muscle) using histamine or metacholine
b. Indirectly (activating mast cells to
release mediators that affect the smooth muscle) such as
exercise or inhaling hypertonic saline.
Whichever
method is used the spirometry is performed before any
provocation and then the challenge is given using an approved
protocol either for increasing concentrations of
histamine/metacholine/saline or a set exercise protocol and then
the spirometry is repeated on numerous occasions either during
the increasing dosage or at intervals after the exercise.
Changes in the FEV1 will be noted and a calculation of the
maximal drop in FEV1 post provocation is recorded and
if there is a reduction a bronchodilator is given and the post
bronchodilator spirometry results are recorded.
Test of
Eosinophilic Inflammation/Exhaled Nitric Oxide Levels
The exhaled
nitric oxide levels may be monitored over a period of time and
in conjunction with sputum eosinophillia counts can have a high
specificity and sensitivity to asthma but is more useful in
assessing the severity of asthma and/or the response to
treatment. These investigations are somewhat more lengthy and
are not routinely used in the diagnosis/treatment of asthma in
USA/UK.